
Trauma vs. Anxiety: How to tell the difference and what to do next
You've been anxious for as long as you can remember. Maybe you've tried therapy before, or maybe you're just now reaching out. Either way, something isn't working. The worry doesn't stop. You can't fully relax. Certain situations send you spiraling in ways that feel completely out of proportion.
And somewhere in the back of your mind, you're wondering: is this anxiety? Or is something deeper going on?
That question matters more than most people realize. Because anxiety and trauma can look almost identical on the surface. They share symptoms, they feed each other, and they often show up at the same time. But they have different roots, different patterns, and they respond better to different kinds of treatment.
If you've been treating one when you actually needed to address the other, you might be working twice as hard and getting half the results.
Here's what you need to know.
Why This Gets So Confusing
Both anxiety and trauma can leave you feeling on edge, avoidant, exhausted, and reactive. Both can make your body feel unsafe. Both can disrupt sleep, concentration, and relationships. So why does it matter which one is driving the bus?
Because the intervention that helps most depends on where the distress is coming from.
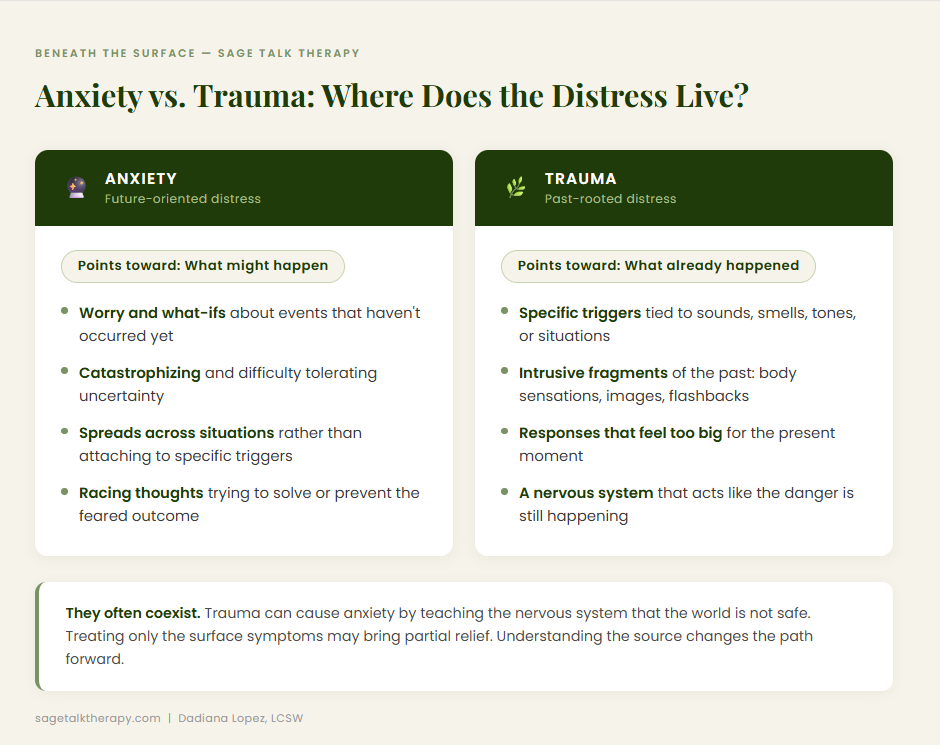
Generalized anxiety tends to be about what might happen. It lives in the future. The anxious mind runs worst-case scenarios, catastrophizes, and struggles to tolerate uncertainty. A person with anxiety might lie awake running through every possible thing that could go wrong at work tomorrow.
Trauma-related distress tends to be about what already happened. It lives in the past that your nervous system hasn't finished processing. A trauma response isn't really about the present moment, even when it feels that way. It's about a past experience that got stored in your body and brain as still happening, still dangerous.
That distinction, subtle as it sounds, changes everything about how you approach healing.
The Overlapping Symptoms (and Why They Overlap)
Before going further, it's worth naming why this is genuinely hard to sort out, even for clinicians.
Trauma and anxiety share a nervous system. Both involve the amygdala, the brain's threat-detection system, going into overdrive. Both can produce racing heart, shallow breathing, hypervigilance, sleep problems, irritability, and the urge to avoid things that feel unsafe. About 80% of people with PTSD also carry at least one other mental health diagnosis, and anxiety disorders are among the most common companions.
Trauma can also cause anxiety. When something painful happens and your nervous system takes it in as evidence that the world is not safe, your baseline threat level goes up. You might develop generalized anxiety, panic disorder, or social anxiety in the wake of a traumatic experience, even without meeting the full criteria for PTSD.
This is part of why people can spend years treating anxiety symptoms and still feel stuck. The anxiety is real. But underneath it, there's unprocessed material the nervous system is still guarding.
Key Differences Worth Paying Attention To
While the overlap is real, there are some meaningful patterns that can help you (and your therapist) start to get a clearer picture.
What triggers the response?
With generalized anxiety, distress tends to spread across lots of situations. It's not always tied to one specific thing. With trauma, there are often particular triggers: a smell, a tone of voice, a specific type of situation, a time of year. The response can feel sudden and intense, and you may notice it doesn't fully make sense to your rational mind in the moment.
How does your body respond?
Anxiety tends to show up as hyperarousal: heart racing, thoughts speeding, the urge to move or fix something. Trauma responses can look like this too, but they can also show up as the opposite. Numbness, shutdown, going flat, difficulty feeling anything. This is called hypoarousal, and it's just as much a trauma response as fight-or-flight. If you swing between these two states, that's important information.
What are the intrusions like?
Anxiety brings worry and "what if" thinking. Trauma can bring actual fragments of the past: flashbacks, intrusive memories, images or body sensations that arrive without warning and feel very present, not historical. You're not thinking about something that happened. You're re-experiencing it.
Where does the story point?
When you track your distress, does it point toward an imagined future or a real past? Trauma-linked distress often connects, even loosely, to something that actually happened. Sometimes that connection is obvious. Sometimes it takes a while to see.
The Nervous System is the Common Thread
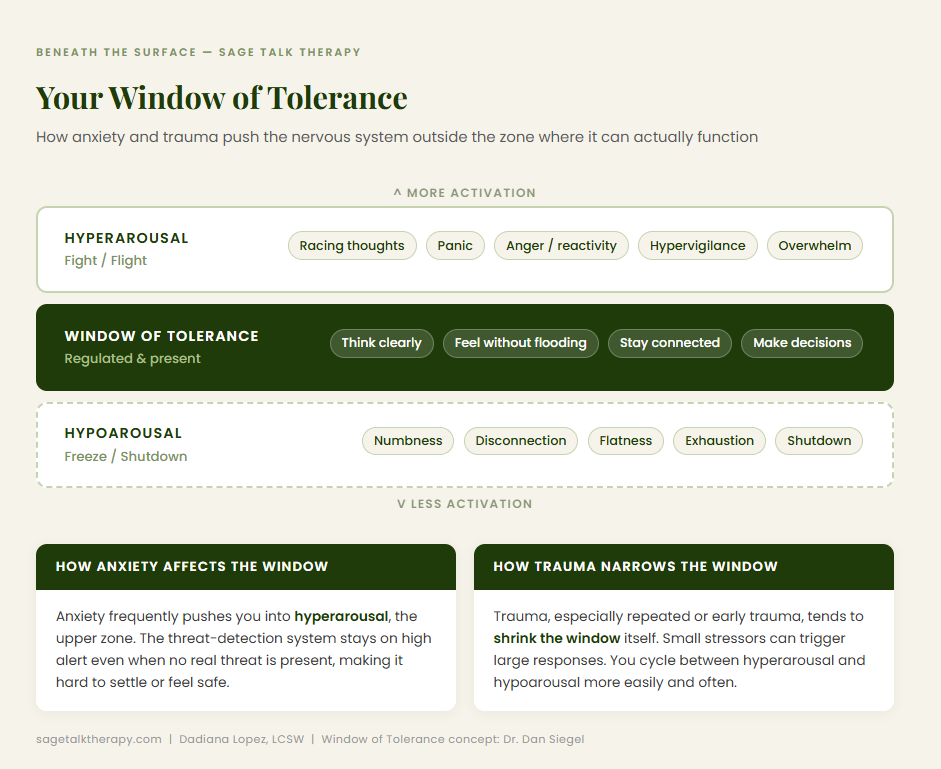
One of the most useful frameworks for understanding both anxiety and trauma is the window of tolerance, a concept developed by psychiatrist Dan Siegel.
Your window of tolerance is the zone of arousal where your nervous system can function effectively. Inside it, you can think clearly, feel your emotions without being overwhelmed, and engage with the world.
Outside it, you go into survival mode.
Hyperarousal: above the window. Panic, racing thoughts, flooding, anger, reactivity. The system is on high alert.
Hypoarousal: below the window. Numbness, disconnection, exhaustion, shutdown. The system has gone into collapse mode.
Both anxiety and trauma can push you outside that window regularly. But trauma, especially repeated or early trauma, tends to narrow the window significantly. Small things can trigger big responses because the nervous system has been conditioned to treat almost everything as a possible threat. With a narrower window, you cycle in and out of dysregulation far more easily.
This is one reason why standard talk therapy sometimes isn't enough for trauma. You can understand your experiences completely and still have a nervous system that acts like the danger is ongoing.
What Actually Helps: The Treatment Picture
Here's the practical piece. Both anxiety and trauma are treatable. You don't have to white-knuckle through either one. But the approach matters.
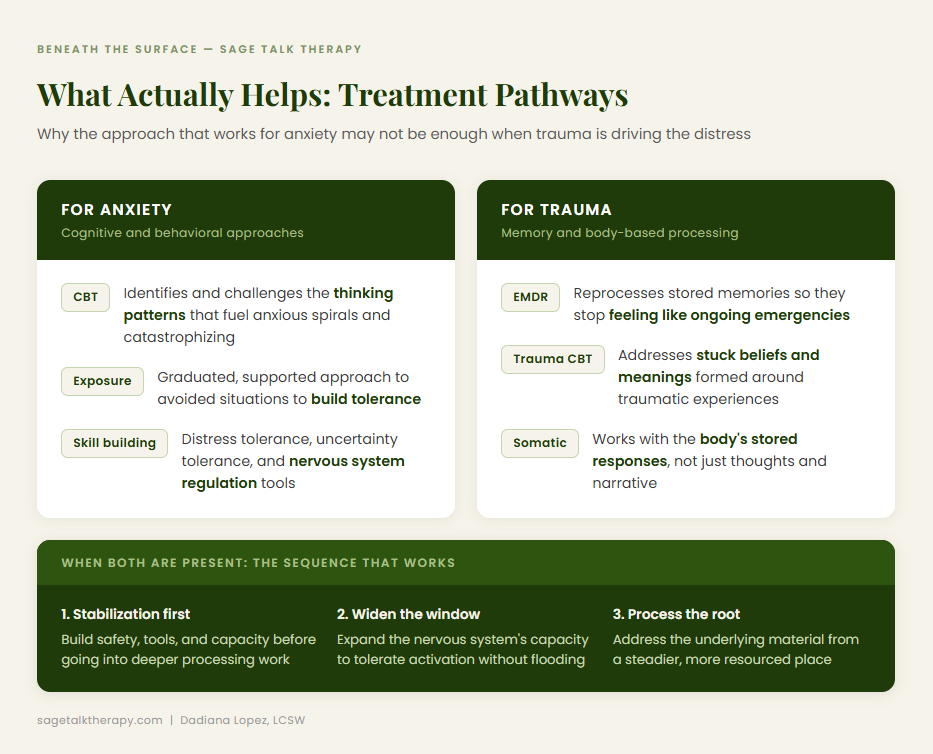
For anxiety, evidence-based treatments like cognitive behavioral therapy (CBT) and exposure-based approaches work well. They help you challenge the thinking patterns that fuel anxious spirals, build tolerance for uncertainty, and approach avoided situations in graduated steps. Medication can also be part of the picture for some people.
For trauma, the research increasingly points toward approaches that work with the body and with memory processing, not just with thought patterns. CBT alone often isn't sufficient. Treatments like EMDR (Eye Movement Desensitization and Reprocessing), somatic approaches, and trauma-focused CBT are specifically designed to help the nervous system finish what it started, process the stored experience, and integrate it so it stops feeling like an ongoing emergency.
EMDR in particular works by helping the brain reprocess traumatic memories so they're stored differently, more like regular memories, with less charge attached. Clients often describe it as the memory still being there but no longer having the same grip. The body stops responding to it as if it's happening right now.
When both anxiety and trauma are present, good therapy holds both. Stabilization comes first. You build capacity. You develop tools for regulation. Then, from a steadier place, deeper processing work becomes possible.
A Note On Complex Trauma
Not all trauma looks like a single, identifiable event. Complex trauma refers to the kind that accumulates over time, often in childhood, often in relationships: neglect, emotional unavailability, chronic criticism, instability, abuse. It doesn't always come with a clear "this is when it happened" story.
People with complex trauma histories often carry deep anxiety that feels like it's just who they are. Constant self-doubt. Difficulty trusting. Hypervigilance in relationships. An overactive inner critic. It can look a lot like a personality trait or a character flaw rather than what it actually is: a nervous system response to chronic conditions.
This kind of history also tends to narrow the window of tolerance significantly. Treatment is slower and more layered. But it's just as possible to heal.
What to Do Next
If any of this is resonating, here are some practical steps.
Get a thorough assessment. Don't rely on a self-diagnosis or a single intake screening. A good therapist will want to understand your history, your symptoms, when they started, what they connect to, and how your nervous system shows up across different situations. That picture takes time to develop, and it's worth developing carefully.
Ask about trauma-informed care. This doesn't mean every session will be about excavating your past. It means your therapist understands how trauma affects the nervous system and will factor that in, whether or not you've identified trauma as the central issue.
Be curious about triggers. When you notice anxiety spiking, see if you can, from a safe distance, get curious about what preceded it. Was there something familiar about the situation? Did your body respond before your mind had time to catch up? These patterns hold information.
Don't rule out EMDR. If you've been in therapy and feel stuck, or if your anxiety has a quality of being too fast and too physical to think your way out of, EMDR might be worth exploring. It was designed specifically for this kind of work.
Give yourself credit for asking the question. The fact that you're trying to understand what's actually happening is not a small thing. Most people spend years managing symptoms without ever digging into their source. You're already doing something different.
YOU DESERVE MORE THAN COPING
Anxiety management is useful. Coping skills matter. But they're not the ceiling of what's possible.
If there's trauma underneath your anxiety, and very often there is, treating only the surface means you're constantly refilling a bucket with a hole in it. The work that addresses what's actually driving the distress is harder. It requires a therapist you trust, a pace that feels safe, and a lot of patience with yourself.
But the result isn't just less anxiety. It's a nervous system that actually knows the past is over. A body that can settle. A life that doesn't have to be organized around managing symptoms.
That's what healing looks like. And it's available to you.
Learn more about Anxiety Therapy.
Learn more about Trauma Therapy.

Dadiana Lopez
LCSW · Anxiety & Trauma Therapist · EMDR Specialist
Dadiana Lopez is a Licensed Clinical Social Worker and EMDR therapist based in White Plains, NY. She specializes in anxiety, trauma, PTSD, and the patterns that form in the wake of both — including people-pleasing, perfectionism, and burnout. She sees clients in person in Westchester and online throughout New York and Connecticut.
Seeing clients in-person in White Plains, NY and online throughout New York and Connecticut.