
Why Therapy Didn’t Work Before
If you've been in therapy before and walked away thinking it just wasn't for you — you're not alone. And you're probably not right.
For a lot of people who end up in trauma-informed therapy, previous therapy wasn't useless. It was often genuinely helpful in some ways. They developed insight, vocabulary, a better understanding of their patterns. They could name what was happening. They understood, intellectually, where things came from.
And they still didn't feel different.
That gap — between understanding and actually feeling different — is not a personal failing. It's a clinical one. It points to a real limitation in certain therapeutic approaches when applied to trauma, anxiety with deep roots, or patterns that formed early in life. The insight was real. The approach just didn't reach far enough.
This post is an honest explanation of why that happens, and what trauma-informed therapy does differently that allows it to reach what conventional approaches often can't.
What conventional therapy does well — and where it stops
Before anything critical, it's worth being clear: conventional talk therapy has real value. Cognitive Behavioral Therapy has strong evidence for a wide range of concerns. Psychodynamic therapy creates meaningful self-understanding. Supportive counseling helps people process difficult life events and feel less alone.
The limitation isn't that these approaches are ineffective. It's that they work primarily through the thinking brain — through conversation, reflection, reframing, and insight. And for many people, especially those dealing with trauma, anxiety rooted in early experience, or patterns that have been in place for decades, the thinking brain is not where the problem lives.
Trauma and deeply rooted anxiety are nervous system phenomena as much as cognitive ones. They live in the body's automatic responses, in the patterns that fire before conscious thought catches up, in the biological encoding of experiences that happened long before there were words for them.
When therapy works only at the cognitive level, it's working on the display rather than the operating system. The display can look cleaner. The underlying code keeps running the same way.
![Where the problem lives" comparison] Alt text: "Diagram comparing where conventional therapy works versus where trauma is actually stored](https://images.squarespace-cdn.com/content/v1/66847f92ca9dcc009453572b/951a45c5-8e50-43c1-997a-6b2139f00255/tdw_visual1_where.jpg)
The most common reasons previous therapy didn't create lasting change
These are the patterns I hear most often from clients who come in having already tried therapy.
It stayed at the surface.
Sessions focused on the week's events, current stressors, and managing symptoms. That kind of support has its place. But if the underlying trauma or nervous system pattern never gets addressed, the support becomes indefinite maintenance rather than genuine change. Every week brings new material because the root keeps generating it.
It relied on insight to produce change.
Understanding why you do something doesn't automatically change the doing of it. This is one of the most frustrating experiences in therapy — developing sophisticated awareness of a pattern while remaining completely unable to stop it. That's not a failure of effort or intelligence. It's the nature of patterns that are encoded below the level of conscious thought.
It moved too fast into difficult material.
Paradoxically, some therapy that tries to address trauma directly can make things worse rather than better — if it moves into trauma processing before adequate safety and stabilization have been built. This is called re-traumatization. The client gets flooded, destabilized, and leaves sessions feeling worse than when they arrived. Over time, they may conclude that the trauma is too much to touch — when the actual issue was pacing, not the material itself.
The relationship wasn't the right fit.
This one is simple and worth saying directly. Therapy is a relational process, and the quality of the therapeutic relationship matters enormously for outcomes — perhaps more than any specific modality. If you didn't feel genuinely safe, seen, or understood, the work was operating with a significant handicap regardless of the therapist's credentials.
The approach wasn't matched to the actual problem.
If chronic anxiety has roots in early relational experiences or developmental trauma, treating it purely as a thought pattern problem misses the root. If perfectionism is fear-driven, CBT alone often isn't enough. If the nervous system is stuck in a chronic threat state, talking about it doesn't settle it. Matching the approach to the actual nature of the problem is one of the most important — and most frequently missed — elements of effective therapy.
What trauma-informed therapy does differently
Trauma-informed therapy isn't a single modality. It's an orientation — a way of understanding how people are affected by their experiences and what they need in order to genuinely heal. Within that orientation, specific evidence-based approaches address what conventional therapy often misses.
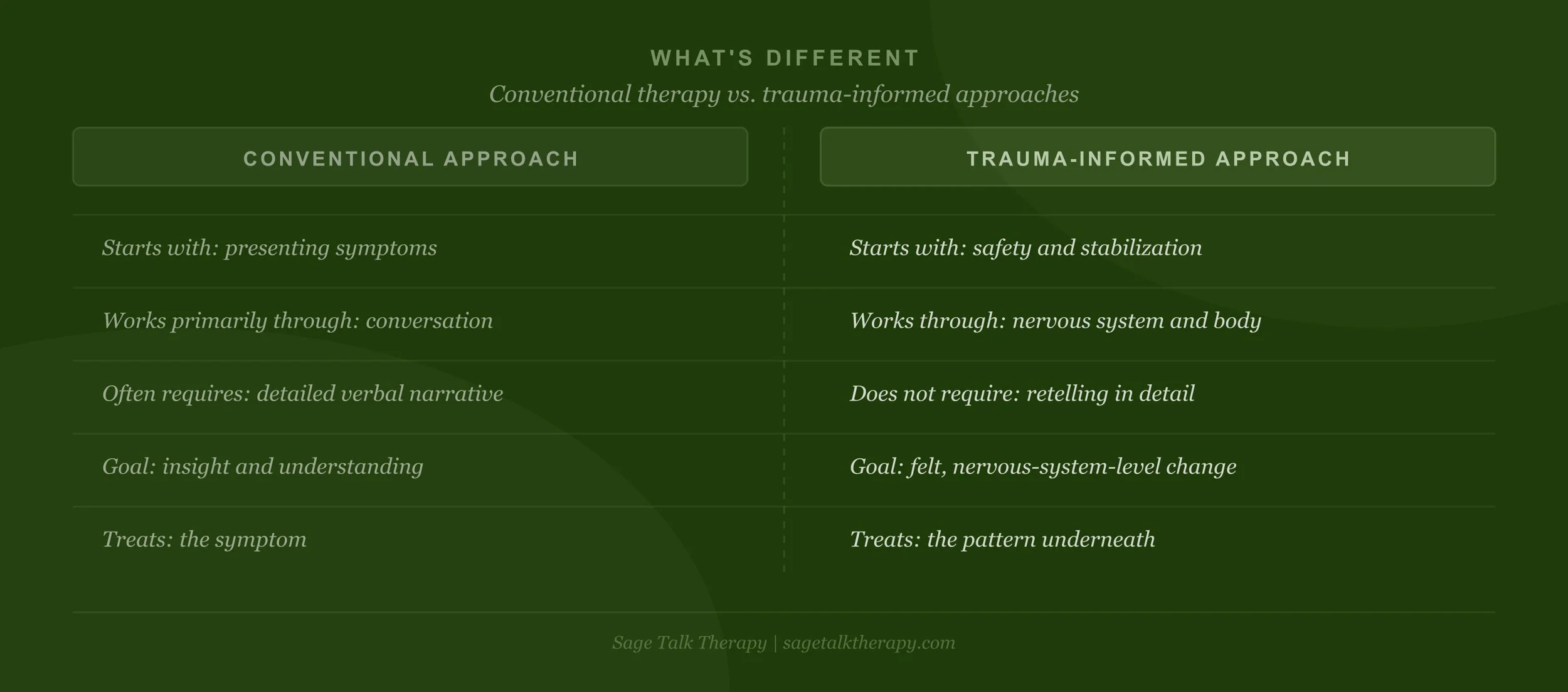
Here is what's different:
It starts with safety, not with the trauma.
Before any processing work begins, trauma-informed therapy prioritizes establishing genuine safety — in the therapeutic relationship, in the client's nervous system, and in the client's daily life. This phase can take weeks or months. It is not a warm-up. It is foundational.
Clients who have experienced previous therapy that felt destabilizing or overwhelming often needed more time here than they received. Rushing toward the material without adequate stabilization produces the flooding and re-traumatization that makes people conclude therapy isn't for them.
It works at the nervous system level, not just the cognitive one.
EMDR, somatic experiencing, and other body-based approaches work where trauma is actually stored — in the nervous system's automatic responses, in physical sensation, in the encoded threat responses that fire without conscious involvement.
This is why clients often describe these approaches as reaching something that years of talk therapy couldn't. Not because talk therapy wasn't doing anything, but because these approaches are working at a different level of the system — one that thinking and talking alone don't access.
It doesn't require you to narrate your trauma in detail.
One of the most common misconceptions about trauma therapy — and one of the most significant barriers to people seeking it — is the belief that healing requires talking through everything that happened in explicit detail.
For approaches like EMDR and somatic experiencing, that's simply not true. EMDR works with the body's reprocessing system rather than verbal narrative. Clients can hold an experience internally without describing it. Many clients process experiences in EMDR that they have never been able to talk about — and find that the processing happens at the nervous system level regardless of how much they put into words.
It treats the pattern, not just the symptom.
Trauma-informed therapy looks for what's underneath the presenting concern. Anxiety is a symptom. Perfectionism is a symptom. People-pleasing is a symptom. Low Self-Esteem is a symptom. Each of these points back toward experiences and nervous system learning that created them. Addressing only the symptom produces temporary relief. Addressing the pattern underneath produces genuine, lasting change.
It's paced to what your nervous system can actually tolerate.
Good trauma therapy moves at the pace of the slowest part of you. It doesn't push. It doesn't flood. It builds the capacity to tolerate increasing levels of activation over time — widening the window of tolerance rather than throwing the client into the deep end and hoping they swim.
The specific approaches and what they reach
EMDR works by helping the brain complete the processing of traumatic memories that got stuck — encoded in a raw, fragmented state that keeps them feeling present rather than past. Through bilateral stimulation, EMDR activates the brain's natural processing system and allows memories to be integrated rather than relived. The result is that what once flooded the system becomes something that can be held without being overwhelmed by it.
Internal Family Systems (IFS) works with the internal protective structures that trauma creates — the perfectionist, the people-pleaser, the inner critic, the part that shuts down. Rather than fighting these parts or trying to override them, IFS builds a relationship with them — understanding what they're protecting, what they're afraid of, and what they need in order to stand down. For many clients this is the first approach that has made their inner experience feel genuinely workable rather than something to be managed or suppressed.
Somatic Experiencingworks directly with how trauma is held in the body — the chronic tension, the automatic shutdown, the hypervigilance that lives in the muscles and nervous system rather than in conscious thought. By bringing attention to physical sensation and supporting the body's natural completion of interrupted survival responses, somatic work reaches the physiological layer of trauma that sits beneath all the cognitive processing.
These approaches are not mutually exclusive. In practice, effective trauma-informed therapy often weaves between them depending on what the client needs in a given session and where they are in the work.
"But I did EMDR and it didn't work either."
This deserves to be addressed directly, because it happens.
EMDR done without adequate preparation and stabilization can be overwhelming rather than healing. EMDR applied to complex developmental trauma without accounting for the level of nervous system dysregulation can produce flooding rather than processing. EMDR with a therapist whose training was insufficient or who didn't understand trauma pacing can feel just as destabilizing as any other poorly paced approach.
The modality matters. The way it's applied matters just as much.
If a body-based or EMDR approach has felt too intense in the past, that's important clinical information — it suggests the preparation phase needed more time, or the pacing needed to be slower, or the stabilization tools needed to be stronger before processing began. It doesn't mean EMDR can't work. It means something in the implementation wasn't calibrated to what your nervous system actually needed.
A trauma-informed therapist will ask about previous therapy experiences specifically because how you've responded to past approaches shapes how we work together from the beginning.
![What to expect from trauma-informed therapy" visual] Alt text: "Three-phase diagram showing what trauma-informed therapy looks like from safety through processing to integration.](https://images.squarespace-cdn.com/content/v1/66847f92ca9dcc009453572b/a49b02d7-4814-4b1b-908b-2d7baa572f70/threelayersv3.png)
what the work actually looks like
Trauma-informed therapy is not dramatic. It's not cathartic in the way movies suggest therapy should be. For many clients it feels quieter than they expected — and more significant.
Early sessions are about getting to know your history and your nervous system. Building the relational safety and stabilization tools that make deeper work possible. Beginning to understand the connection between what happened and how your system learned to respond.
When processing work begins, it happens gradually. Sessions have a clear structure — preparation, processing, closure — so you never leave destabilized. Between sessions, the work continues in a quieter way as the nervous system integrates what was processed.
Over time, clients describe a felt sense of things shifting rather than a single breakthrough moment. The triggers that used to be overwhelming start to feel more manageable. The patterns that felt automatic start to have more pause before them. The relationship with the past starts to change — from something that feels present to something that actually feels like the past.
This is what it means to heal from trauma. Not the absence of the memory. Not the erasure of the experience. The felt sense, at a nervous system level, that it's over — and that the present moment is genuinely different.
if previous therapy left you skeptical
That skepticism is reasonable and worth honoring. It means you tried, it didn't work the way you hoped, and now you're weighing whether to try again.
What I'd offer is this: the fact that one approach didn't produce the results you needed tells you something specific about that approach. It doesn't tell you that change isn't possible. It doesn't tell you that the problem is too entrenched. It doesn't tell you that you're somehow beyond help.
It tells you that the method didn't match the problem.
If you're based in Westchester or anywhere in New York or Connecticut, I'd welcome the chance to talk through what previous therapy looked like for you, what you're still carrying, and whether a trauma-informed approach might reach what hasn't been reached yet.
Learn more about trauma therapy.
Learn more about EMDR Intensives.

Dadiana Lopez
LCSW · Anxiety & Trauma Therapist · EMDR Specialist
Dadiana Lopez is a Licensed Clinical Social Worker and EMDR therapist based in White Plains, NY. She specializes in anxiety, trauma, PTSD, and the patterns that form in the wake of both — including people-pleasing, perfectionism, and burnout. She sees clients in person in Westchester and online throughout New York and Connecticut.
Seeing clients in-person in White Plains, NY and online throughout New York and Connecticut.